Updated on Monday - August 28, 2017 almost a week later.
Continuing on the above:
I have always been a firm believer that pain must be endured, even if it is gut wrenching and you literally are in tears. Painkillers and steroids are harmful, they ruin your body, destroy you immunity, cause unexpected side effects - those were the logical reasons I gave myself. I also felt that giving in to pain was a sign of weakness, you fight pain not surrender!
A very good approach, both reasonable and logical, but the question I started asking myself is, up to what point? At what Threshold of pain do you break your limit of tolerance?
Let us now go over for some scientific jargon:
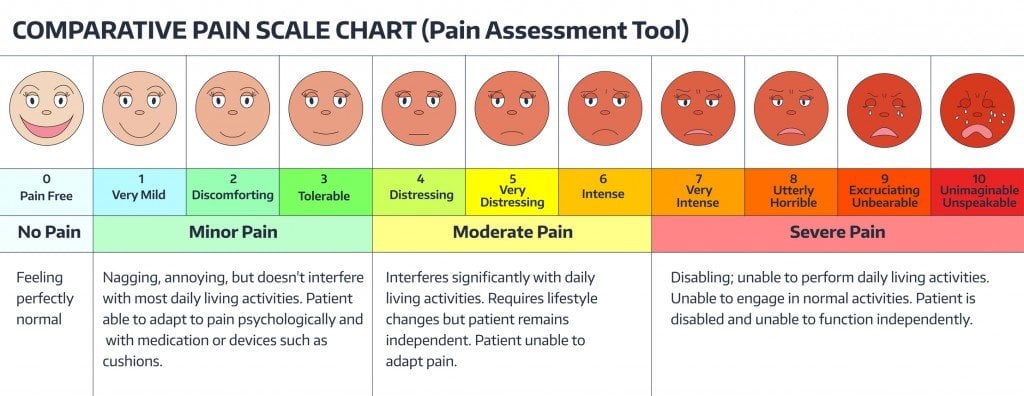
The threshold of pain or pain threshold is the point along a curve of increasing perception of a stimulus at which pain begins to be felt. It is an entirely subjective phenomenon. A distinction must be maintained between the stimulus (an external thing that can be directly measured, such as with a thermometer) and the person's or animal's resulting pain perception (an internal, subjective thing that can sometimes be measured indirectly, such as with a visual analog scale). Although an IASP document defines "pain threshold" as "the minimum intensity of a stimulus that is perceived as painful",[1] it then goes on to say (contradictorily in letter although not in spirit) that:[1]
Traditionally the threshold has often been defined, as we defined it formerly, as the least stimulus intensity at which a subject perceives pain. Properly defined, the threshold is really the experience of the patient, whereas the intensity measured is an external event. It has been common usage for most pain research workers to define the threshold in terms of the stimulus, and that should be avoided ... The stimulus is not pain (q.v.) and cannot be a measure of pain.
Although the phrasing may not convey it perfectly, the distinction clearly meant is the aforementioned one between the stimulus and the perception of it. The intensity at which a stimulus (e.g., heat, pressure) begins to evoke pain is thus called by a separate term, threshold intensity. So, if a hotplate on a person's skin begins to hurt at 42C (107F), that is the pain threshold temperature for that bit of skin at that time. It is not the pain threshold (which is internal /subjective) but the temperature at which the pain threshold was crossed (which is external/objective).
The intensity at which a stimulus begins to evoke pain varies from individual to individual and for a given individual over time.
Pain tolerance is the maximum level of pain that a person is able to tolerate. Pain tolerance is distinct from pain threshold (the point at which pain begins to be felt). factors that affect pain tolerance are association and disassociation. These two cognitive strategies have been found to increase pain tolerance. It is widely believed that regular exposure to painful stimuli will increase pain tolerance: increases the ability of the individual to handle pain by becoming more conditioned to it. However, in some cases, there is evidence to support the theory that greater exposure to pain will result in more painful future exposures. Repeated exposure bombards pain synapses with repetitive input, increasing their responsiveness to later stimuli, through a process similar to learning. Therefore, although the individual may learn cognitive methods of coping with pain, such methods may not be sufficient to cope with the boosted response to future painful stimuli. "An intense barrage of painful stimuli potentiates the cells responsive to pain so that they respond more vigorously to minor stimulation in the future."
Thus, trauma victims (or patients in pain) are given painkillers (such as morphine) as soon as possible to prevent pain sensitization.
~Source: Wikipedia~
So from the above it can be deduced that Threshold of pain is that point where you start to feel the pain and the Tolerance limit is when you admit you feel the pain and submit to it.
Most of us, at least me, during my Asthma attacks would try to keep as much as a distance between the pain threshold and pain tolerance, for reasons, well, given above?
So why the change in my stance?
For that you, my reader would have to understand what happens to my body once the pain threshold is breached till the time I give in.
During an asthma attack, the muscles that surround the bronchial tubes constrict, narrowing the air passages and making it extremely difficult to breathe. Worsening airway inflammation causes the muscles wrapped around airways (bronchiolar muscles) to spasm, constrict, and squeeze airways. The combination of bronchospasm and mucus hyper secretion creates airway obstructions, or narrowed airways. Obstructed airways act as a barrier that resists, or acts to prevent, the flow of air out of the airways (meaning, during exhalation). This increased resistance thereby slows the movement of air during exhalation. This makes it so that you can take in air, although your exhalation is prolonged. Your next breath may come before exhalation is complete. When the next breath comes before the current breath is complete, this causes air to become trapped inside your chest. When you inhale, it may feel like you can't take in a complete breath.
When you cannot exhale completely, air can become trapped inside your chest to the point it is fully expanded, thereby giving the appearance of a barrel. This occurs when your lungs or over-inflated with air, making your chest appear to be larger than normal (over expanded). You have to sit with hunched shoulders, elbows locked for your shoulders will be elevated as high as you can get them, in an effort to create more room to suck in air. And you also use your accessory muscles (chest / shoulders, diaphragm), These are muscles that are not normally used for breathing, and most are used to assist with inhalation. When your intercostal muscles and diaphragm need assistance getting air through obstructed and narrowed airways due to increased resistance, these muscles are used. They are used in an effort to suck more air into your chest.
To make it simpler for you to understand, just imagine running five flights of stairs, upstairs, walk two more (no breaks) and then continue on the eight flight up. That should give you an idea of the breathlessness that an asthma patient has, continuous, even when sitting. And sleeping, even leaning back is impossible. You cannot breathe. Period. Nothing matters! What can one do when one cannot breathe?
I have fought these attacks (almost one each year, lasts for a week to ten days the breathlessness goes away in a few days, but being able to walk at least half a kilometre without gasping takes at least three weeks, provided I do not have a relapse. The lesser the time gap between attacks, the harder the recovery).
Finally, I had an epiphany, each time I forced my body to fight without assistance (painkillers, steroids or antihistamines) I was actually torturing my muscles, pushing them to beyond endurance levels. And I was in risk of causing airway fibrous, which is an irreversible condition, a permanent damage to the airways. The alternate is to take a continuous medication, which is primarily steroids (oral or inhalers), which when steroid tablets are taken for many months or years, harmful side effects are likely and almost inevitable. The list of possible effects is long; it includes mood changes, forgetfulness, hair loss, easy bruising, a tendency toward high blood pressure and diabetes, thinning of the bones (osteoporosis), suppression of the adrenal glands, muscle weakness, weight gain, cataracts, and glaucoma. After being swallowed, these tablets are absorbed from the stomach into the bloodstream and taken not only to the bronchial tubes (to treat asthma) but also to every other part of the body. Their effects are widespread.
So here is your choice destroy your lungs by not taking an medication, because you have over worked those muscles or ruin your body with steroids? Not a pleasant choice. But then is there no middle way, an optimisation?
Turns out there is and how to go about it is your choice.
I choose to go in for an intensive treatment at the time I had my attack, the doctor took a look at me and suggested that I should be admitted to the ER, immediately. He did not force me, because I almost burst into tears and looked murderous (I scared him good). So he took a PEAK test, the standard is 350, I gave an abysmal result of 90 after three attempts. (The peak expiratory flow (PEF), also called peak expiratory flow rate (PEFR) is a person's maximum speed of expiration, as measured with a peak flow meter, a small, hand-held device used to monitor a person's ability to breathe out air. It measures the airflow through the bronchi and thus the degree of obstruction in the airways.)
Then he packed me off to the ER, suggested four continuous sessions of nebulisation, with 10ml of Duolin, prescribed a week course on inhaler, a two week course of muscle relaxant. The first session of nebulisation, had me eating my brother's ear off, who was so happy that I could breathe to talk, heard me with a goofy grin throughout. Second round, I slept, leaning back (on my second day of attack). Third round, I was hungry and listing the items I was planning to eat over the next few hours and the fourth time, I actually thought of running home. It was a miracle; I never thought I could recover from an attack so quickly.
Today, a week later, I am back at work. During last week, I managed to complete my update of my on going update, post a new story, make two new threads and also did a few PS, the old me fighting it with medication, would still be wheezing (did I tell you that you cannot eat properly, because a full stomach would mean restricted diaphragm movement and hence you are unable to breathe?)
So now, once this course is over, I will discontinue those medications, but I have learnt from this experience. I am going to invest in a PEF meter, learn specific lung strengthening exercises and measure the airflow and keep the inhaler as an emergency standby with the nebuliser at easy reach. I can prevent the attack from being full blown with one session of nebulisation; maybe use half the dosage, thus doing away with the need to use of antihistamines.
I think I truly rambled here, but what I wanted to say was, make an informed choice, and learn all the pros and cons before rejecting anything. Tolerating pain far and beyond the threshold of pain could be far more dangerous over a prolonged course of time than treating pain with steroids could be. A balanced approach is always possible.
Note - this is only from my personal experience, is not and cannot be a substitute for medical advice.